Hadi ilk önce şu oruç meselelerine bakalım, merak etmeyin bütün cevaplara ve becerilemeyen demagojiye(tecrübeli siyasetçiler hariç yapabileni görmedim zaten) cevap vereceğim :
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5819235/
Öncelikle bu denetimin ne koşullara sahip olduğu :
"
TNHC (
www.truenorthhealth.com) is an integrative medical facility in Santa Rosa, CA, USA that offers a residential health education program specializing in water-only fasting and dietary intervention. Patients in this study had access to medical, naturopathic, and chiropractic doctors. Private rooms, 24-h medical supervision, and daily educational activities were also provided.
"
Anlamlandırmamıza yardımcı olması için:
"
Abbreviations
AE Adverse event
CI Cumulative incidence
CTCAE Common Terminology Criteria for Adverse Events
ECI Estimated cumulative incidence
HGAE Highest grade adverse event
HLT Highest level term
IQR Interquartile range
IV Intravenous
LLT Lowest level term
MedDRA Medical Dictionary for Regulatory Activities
SAE Serious adverse event
SOC System organ class
TNHC TrueNorth Health Center
VAS Visual analog scale
"
"
Adverse event identification and coding
Data on AEs were collected from clinical chart notes of self-reported symptoms, clinical and diagnostic findings, and medical management of symptoms. Laboratory values were not systematically included due to data incompleteness. The CTCAE (v4.03) scale was used to grade AE severity: AE1 – mild, AE2 – moderate, AE3 – severe, AE4 – life threatening or disabling, and AE5 – death. AEs were characterized using the MedDRA (v12.1) terminology according to the system organ class (SOC), which uses the highest level term (HLT), including anatomical or physiological system, etiology, and/or purpose, and the lowest level term (LLT). Pain-related AEs, reported on a visual-analog scale (VAS) from 0 to 10, were reported as follows: AE1 = VAS 1–4, AE2 = VAS 5–7, and AE3 = VAS 8–10 [
42,
43]. A serious adverse event (SAE) was determined based on the definition used by the Department of Health and Human Services [
44]. A codification guide was created to ensure that there was consistent codification of AEs. A single trained clinician (J.S.F) identified, reviewed, and classified AEs, according to the above criteria, for each daily entry in the electronic chart note. A user interface within the relational database (MS Access) was used for direct data entry of the codified data. One week after the conclusion of data abstraction, intra-rater reliability was assessed based on a random sample of daily logs. The dataset is available from the Dryad repository, 10.5061/dryad.6cg6j.
"
"
Adverse event descriptive analysis
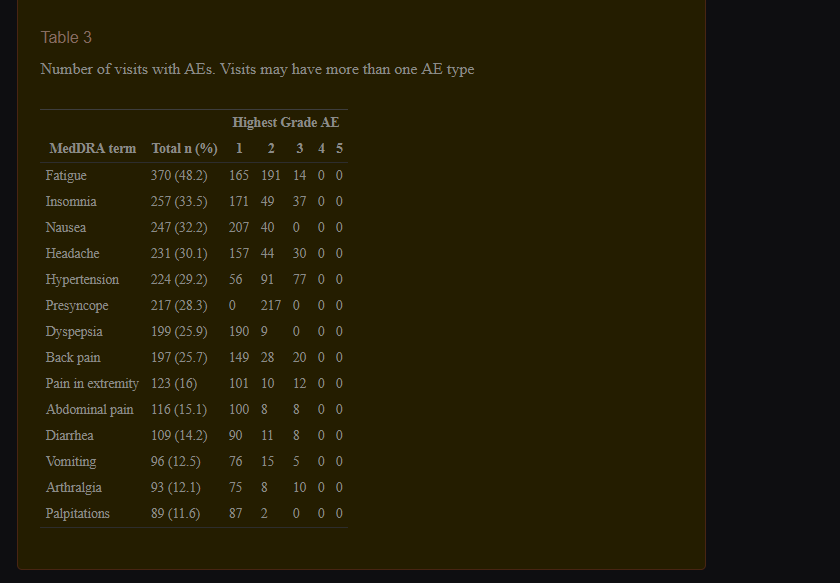
Visits were stratified by water-only fast length: 2–7 (short), 8–14 (medium), 15–21 (long), or 22+ (extended) days. These categories were chosen to represent lengths of typical fasts. Within visits, days were grouped by fasting and refeeding status. Summary statistics of the study population at the patient and visit levels were tabulated. Chief complaints were categorized by SOC when possible. For each visit, the highest grade AE (HGAE) experienced (of any MedDRA term) and the total AEs were calculated for the fasting, refeeding, and entire protocol periods. Tallies and percentages of HGAE within each of these periods were computed in total and by the fasting length strata. Spearman’s correlation between fasting length strata and HGAE was computed using integer scores for the fasting length strata. For each MedDRA term, counts and percentages of visits with at least one AE of a term were computed for each AE grade and for all AE grades combined. Similar counts and percentages were computed for individual AEs without taking visits into account. We report MedDRA terms that were experienced in more than 10%. Association between a visit’s HGAE and age was assessed graphically and measured with Spearman’s correlation [
46]. An association between HGAE and gender was tested using a two-sided Fisher’s exact test. The paired difference in HGAE during fasting versus refeeding was tested using a paired t-test. Kaplan-Meier estimates of cumulative incidence (CI) were computed for each category of fasting length for the following AE categories: any AE, any AE ≥ 2, and any AE ≥ 3 [
47]. All AEs of grade 3 or higher were carefully reviewed (A.C.G., T.R.M, J.S.F.), and SAEs were further described by brief narrative. Analyses were performed in R 3.1 using the survival, [
48,
49] irr, [
45] ggplot2, [
50] dplyr, [
51] and htmlTable packages [
52].
"
Ve:
"
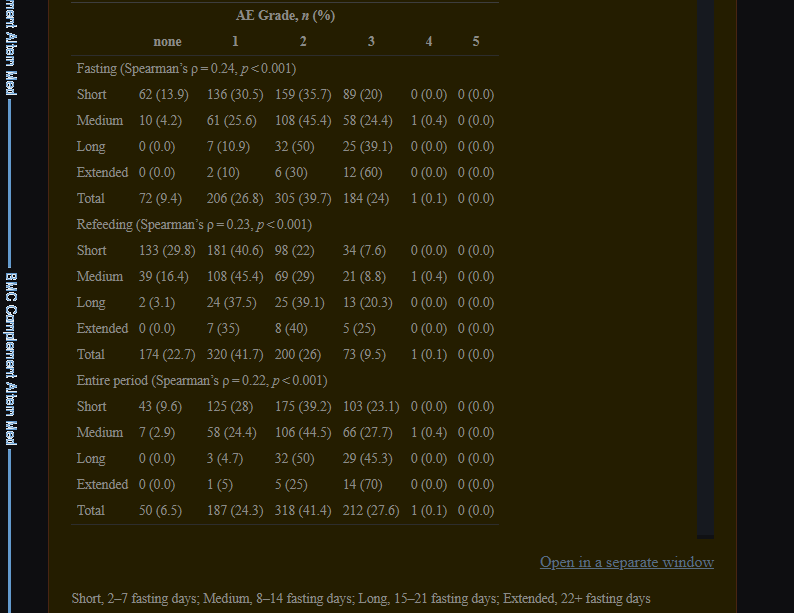
AEs were classified on a graded scale of 1–5 according to CTCAE (v4.03) and MedDRA (v12.1) criteria (see
Methods). HGAE experienced during the fasting, refeeding, and entire protocol period of each visit is presented in Table
2. During the entire protocol period (i.e., fasting and refeeding) for all visit lengths, the HGAE experienced in the majority of visits (
n = 555, 72.3%) was grade 2 or lower and in 212 visits (26.6%) it was grade 3. There was a weak positive correlation between fast and refeed length and HGAE (Table
(Table2).2). There was 1 patient with a grade 4 AE during a medium visit. There were no deaths (AE5) during any visits. There was a weak positive correlation between HGAE and fast duration (Spearman’s ρ = 0.28,
p = < 0.001) and a weak positive correlation between HGAE and age (Spearman’s ρ = 0.11,
p = 0.002) (Additional file
1: Figure S1a, b). There was no correlation between HGAE and gender (
p = 0.628) (Additional file
1: Figure S1c). During refeeding, the mean HGAE was 0.56 less than during fasting (paired t = − 16.28,
p = < 0.001).
"
Bahsettiğimiz konunun, "aman 10 saat bile yapma geberip gidersin, öldürür bu adamı" gibi bir durum yok ancak bu kadar denetimin içinde :
AE 4 yani yukarıda belirttiğim gibi "AE4 – life threatening or disabling" görülmüş ve AE-2 ve üstü azımsanacak bir miktar değil bence ki hatırlatırsak "AE2 – moderate, AE3 – severe"
"
There were two (0.002% of visits) SAEs that required hospitalization. One was a grade 3 dehydration event that occurred on fasting day 3 in a 73-year-old, male patient. The patient developed headache, fever, and increased blood pressure. He was taken to an emergency facility, where he received antibiotics for potential upper respiratory infection and intravenous (IV) electrolytes for dehydration and was kept under inpatient observation for 3 days. The patient fully recovered and returned to TNHC. The other was a grade 4 hyponatremia event that occurred on fasting day 9 in a 70-year-old, male patient. The patient developed difficulty with speech and was immediately transported to an emergency facility by ambulance. Upon evaluation at the emergency facility, the patient was diagnosed with hyponatremia, administered IV electrolytes, and kept under inpatient observation for 4 days. The patient fully recovered but did not return to TNHC.
"
Background
Modern humans evolved to survive periods of food shortage and have voluntarily fasted for at least 2000 years. Fasting is broadly defined as the voluntary abstinence of some or all caloric foods and beverages for therapeutic, spiritual, or political reasons [
1]. In the last century, research in animals and humans has uncovered several potentially health-promoting physiologic responses to fasting including ketogenesis, hormone modulation, reduced oxidative stress and inflammation, and increased stress resistance, lipolysis, and autophagy [
1–
4]. Clinical research in humans also indicates that fasting improves hypertension, [
5,
6] rheumatoid arthritis, [
7] cardiovascular disease, [
8,
9] metabolic syndrome, [
10,
11] osteoarthritis, [
12] fibromyalgia, [
13] chronic pain, [
14] and quality of life [
15].
Wilhelmi de Toledo et al. recently reviewed several fasting methods and established the first peer-reviewed therapeutic fasting guidelines in English (revision of the 2002 German publication [
16,
17]). The guidelines specify indications, contraindications, and methods for safe implementation and are based on the Buchinger Method (a modified diet supplying 250–500 kcal/day in the form of vegetable broth, fruit and vegetable juices, and honey). The guidelines are also largely applicable to water-only fasting, which is defined as the complete abstinence of substances except for pure water [
18] and is an established method of therapeutic fasting [
1–
3,
19,
20]. Yet it is only briefly described by Wilhelmi de Toledo et al. as a “zero calorie diet” that has not been practiced since the 1970s, when it was primarily used for weight reduction [
17].
Therapeutic water-only fasting research did decline following a period in the 1960s and early 1970s when the method was used as an obesity treatment, [
21–
24] in part due to reports of serious complications, including death, in some fasting subjects [
25–
30]. During this time, it was common to arbitrarily implement fasts lasting 60 days or longer [
29,
31,
32] and to administer chemical compounds to facilitate prolonged fasts. [
25,
28,
33,
34]. Additionally, physicians and researchers did not always screen subjects for contraindications, terminate fasts upon complication, or properly refeed subjects, [
25,
26,
28,
29] all of which are necessary for the safe implementation of water-only fasts [
1–
3]. Therefore, it is difficult to conclude if water-only fasting is inherently dangerous or if the complications were caused by unintentionally harmful fasting practices.
Despite the documented decline in fasting research and contrary to claims by Wilhemi de Toledo et al., [
17] water-only fasting was not entirely discontinued in the 1970s. It has since been utilized for many therapeutic purposes such as the treatment of hypertension, [
5,
6] cardiovascular disease, [
9] appendicitis, [
35] follicular lymphoma, [
36] and as an adjunct to chemotherapy [
37]. Importantly, previous therapeutic implementation and clinical research led to the development of a water-only fasting protocol (see
Methods) that safeguards against serious complications and minimizes minor reactions [
1–
3]. Nevertheless, there is a lack of objective, peer-reviewed data on the safety of water-only fasting.
Therefore, we were motivated to systematically assess the safety of medically supervised, water-only fasting. To this end, we reviewed and characterized the adverse events (AEs) experienced by patients who water-only fasted at TrueNorth Health Center (TNHC) over a five-year period using Common Terminology Criteria for Adverse Events (CTCAE v4.03 [
38]) and Medical Dictionary for Regulatory Activities (MedDRA v12.1 [
39]). We report the severity, frequency, and nature of patient AEs that occurred during this time.
"
Overall, our data indicate that the majority of AEs experienced during medically supervised, water-only fasting are mild to moderate in nature and are known reactions to fasting. This suggests that the TNHC protocol can be safely implemented in a medical setting with minimal risk of a severe or SAE. This study also provides a basis by which further research into the safety and efficacy of this intervention can be conducted.
"
Araştırma iyi ve kötü, kötü olacaksa ortaya çıkan sonuçları güzel bir şekilde incelemiş bazılarını da örnek göstermiş ancak TIBBİ DENETİMDE yapılıyor araştırmalar, burada özellikle şunu vurguluyorum :
İlla yapılacaksa mevcut ise en azından doktora gidip doktorun görüşü sorulmalı.
-------------------------------------------------------------------------------------------------------
Şimdi gelelim Dr.Jason Fung'un bahsettiği şeye, Mr.Jason uzun süre yapılan diyetlerde metabolizma yavaşlamasını çözülemeyen bir mit gibi sunmuş, oysa ki bunun çözümü çok basit ki uzun yıllardır Vücut Geliştirme camiasında bilinir : "Çok uzun süre Definasyon yapılamaz, uzun vadede bir definasyon amaçlanıyorsa 3-4.ayda ve 5-6.ayda (duruma göre) kısa bir zaman için Bulk'a yönenilir ki metabolizma düzene girsin"
Makro miktarları tamamen yok edilmedikçe, kısa zaman dilimi için (1-2 hafta gibi) 600-700 kalori kısımına karşı değilim ancak tamamen aç kalmak bambaşka bir durum yukarıdaki araştırmayı da referans göstererek tekrar tekrar yineliyorum "Doktor görüşü alınmalı"
-------------------------------------------------------------------------------------------------------
Diyemeyiz ancak :
Bilimsel dayanağı olmayan saçmalıklardan bir tanesi bu, bu gibi yazıları görerek gerek hasta insanlar gerek sağlıklı insanlar bir fayda sağlayabileceklerini zannediyorlar sonra sonuç oradaki kadın gibi oluyor. Hatta bu sözler saçmalıktan da öte, sağlık yönünde bir öneri verirken dikkatli olunmalı her insanın yaşı-cinsiyeti-boyu-hastalıkları-geçirdiği hastalıkları-kan değerleri-hormonal değerleri bir değil bir sürü değişken var ve bu kadar değişken ancak bir doktor eşliğinde kontrol edilip analiz edilebilir, üfürükçülerle değil.
---------------------------------------------------
Şimdi gelelim tam bir facia şeklinde olan demagojiye :
Şimdi mesajımı inceleyelim :
Bilimsel saçmalıktır yazmışım DİNSEL saçmalıktır yazmamışım, dinsel herhangi bir öge yok mesajın içinde şimdi konuyu açan üyenin konusunu inceleyelim :
Başlık
"
Water Fasting (Su Orucu) yapan var mı?
"
Su orucu ile dini orucu nasıl bir tuttun merak ediyorum ? Acaba hiç dini bir oruç tuttun mu onu da merak ettim şimdi ?
Devam edelim :
Mesajımı dön tekrar oku "Yapmayacaksın, izin vermem" gibi saçma sapan bir ithaf var mı ? YOK, ister forum olsun ister başka bir yer hakaret olmadığı müddetçe İFADE ÖZGÜRLÜĞÜ denen bir şey vardır, ha dersin "bence bu adam bana sövüyor" o zaman yönetime bildirirsin, uygun görürlerse işlem yaparlar. Burada ister a kişisinin üslubuyla konuşurum, ister çocuk üslubuyla, ister ergen, istersem akademik bir üslupla konuşurum, üslubu mu uygun görmediğini söylemek dışında bir yaptırımda bulunamazsın.
Burada haddini bilmesi gereken ben değilim sensin, konuyu alakası olmayan bir dini boyuta çekerek(ki konu sahibi de belirtmiş) amatörce demagoji yapmaya çalışıyorsun.
Devam edelim :
@respect2us.23 Adamın eskisi kadar burada durmamasına şaşmamalı, kim bilir neler çekti.
") tartıldığımda 90.6 kilo çıktım. Bakalım ilerleyen günlerde ne olacak.
tartıldığımda 90.6 kilo çıktım. Bakalım ilerleyen günlerde ne olacak.  Hele hele birde spor yapılıyorsa düşünemiyorum bile bu nasıl bir bilimsel saçmalıktır
Hele hele birde spor yapılıyorsa düşünemiyorum bile bu nasıl bir bilimsel saçmalıktır